By Otto Yang, April 26, 2020 (Via FB) There has been a lot of speculation and interest recently about antibody testing and the hope that such tests can predict that people are protected from re-infection. People have been bandying about the term "immunity passport" and suggesting that we can monitor antibodies to tell us about herd immunity. However, the WHO just a couple of days ago issued a statement warning against this, saying that there is no evidence for this strategy. I definitely agree, and will take that a step further here, and will explain why. First, regarding the tests, currently very few of them are reliable measurements. Lots of companies and persons of varying integrity (i.e. some are total charlatans) have been pushing their antibody tests on the public, and the public has been gobbling them up. The desire to be tested, understandably, has been frenzied. In this setting, the FDA has pushed through unreliable tests; the fingerstick assay upon investigation by careful academic labs appears to be about 70% accurate.... and some tests out there are far worse (if not completely fake) and not FDA approved. People are charging hundreds of dollars cash only for these tests. To my knowledge so far, the best test is one developed by a group at Mount Sinai, by Dr. Krammer et al. This test has been carefully designed and validated. Many academic medical centers are using a version of this test, including ours. My lab has taken their protocol and confirmed it; in our hands it appears to be highly accurate (comparing the blood of about 40 recovered persons and 100 persons sampled before the pandemic). Based on our results, we are screening recovered persons for plasma donation for antibodies to treat sick patients. We're working on a shoestring budget; I personally drew the blood that we tested for the first several plasma donors (but that politics of science and funding, and the disappointing reasons we haven't had financial support to do this important work are a topic for another time). At any rate, I believe this test overall will be the gold standard; kudos to Krammer et al not only for developing it, but immediately sharing it with the whole scientific community rather than keeping it private for financial gain. OK, so assuming we have good antibody testing available soon, why doesn't that mean we can clear people for immunity passports? The simple answer is that we don't know if having antibodies predicts a protection from infection again. News reports (not formal scientific reports yet) from South Korea and China are suggesting that people who have recovered from infection are getting sick again within several weeks, and their nasal swab PCR tests that were negative after recovery are positive again. It's not entirely clear whether this is a flare up of their prior infection or a new infection with the same virus, but that distinction isn't that important for the purpose of public health policy. Either way, a recovered person can spread the virus again; they are NOT immune. South Korean estimates (unconfirmed) quoted in the press are about 5-10% of recovered persons. I don't know if these persons were tested for antibodies, but pretty much everyone we have tested in my lab have antibodies, although the amount is variable. The immune system has many components, of which antibodies are only one. Very important for viral infections is "cellular immunity," consisting of T cells, further subdivided into CD4 T cells (the ones destroyed by HIV leading to AIDS) and CD8 T cells (so-called killer T cells that patrol the body for virus-infected cells and cancerous cells, seeking them out and killing them). These are difficult immune responses to measure that only highly specialized laboratories pursue (my lab has studied CD8 T cells and their role in HIV infection for over 20 years); they do NOT parallel antibodies. Moreover, there are other complex parts of the immune system, including regulatory cells, innate "memory," etc that we still don't understand very well. Finally, even antibody responses have subtleties; within the response, some antibodies may be "neutralizing" and act against the virus, while others can even be "enhancing" and help the virus get into cells. So is this all just handwaving theory? No; there are concrete examples. If SARS-CoV-2 causes a chronic infection (for now we assume it is cleared out of the body like most respiratory viruses, but that's not 100% certain), then antibodies may do little. Antibodies contribute little or nothing to controlling chronic viral infections such as HIV, hepatitis B and C, cytomegalovirus, herpes simplex viruses, epstein-barr virus; those are almost exclusively contained by cellular immunity (although only partially in the case of HIV). If SARS-CoV-2 is not a chronic infection, it's still not clear that antibodies provide lasting protection, either because they are ineffective or wane quickly over time. Some really interesting experiments a few decades ago took volunteers and infected them with Coronavirus-229E, a virus that causes the common cold in healthy persons. 15 volunteers who already had detectable antibody against this virus were intentionally exposed, and 10 of these got infected. The remaining 5 who didn't get infected were exposed to virus a year later, and all 5 got infected. Thus, antibodies (even accurately measured) are not an "immunity passport" if this coronavirus behaves similarly. This also bodes poorly for a vaccine, if people get reinfected in such a short time. Just about all our vaccines are against infections where survivors of natural infection have durable protective immunity. The vaccine just mimics the natural infection to stimulate the immune system to do what it does normally against the virus. People recover from measles, smallpox, even Ebola and are protected from getting infected again, so a vaccine just needs to copy that process without causing the actual disease. This breaks down when natural immunity fails. The glaring example is HIV; natural immunity generally fails to clear HIV infection, so a vaccine that makes a normal immune response against HIV will also fail because it's copying a failing process. I'm sorry to be the bearer of this potentially negative news. I certainly could be wrong. We just don't know for sure yet if SARS-CoV-2 behaves like its cousin CoV-229E, and I definitely hope it doesn’t. If it does, immunity passports, herd immunity, and possibly vaccines will be failed prospects for containing the pandemic, and we will have to rely on more innovative approaches, like medications (that effectively prevent or treat infection) or artificial immunity through monoclonal antibodies. (The original post can be found here https://www.facebook.com/otto.yang/posts/10157537736124227)
COVID-19, Antibodies, and Immune Protection from Infection
Related



Stay up to date
Get new posts from Roseburg Tracker in your inbox.
More Stories
In Memory of John Lindsey
John Payne Lindsey, 79, of Roseburg, Oregon, was unexpectedly called home to heaven on Dec. 12, 2025, surrounded by his family. John was born March 19...
2 min read
Roseburg Man Charged With Murder of 11-Month-Old Son
DOUGLAS COUNTY, Ore. – A Roseburg man is in custody tonight charged with the murder of his 11-month-old son. On Sunday, March 15, 2026, shortly befor...
2 min read
K9 Nike to Retire From Winston Police Department
Winston Police Dog Retires After Eight Years of service.
1 min read
Roseburg Cuts Ribbon on New Outdoor Tennis and Pickleball Facility
Roseburg’s rebuilt outdoor Stewart Park complex is now open with eight tennis courts and 10 pickleball courts.
3 min read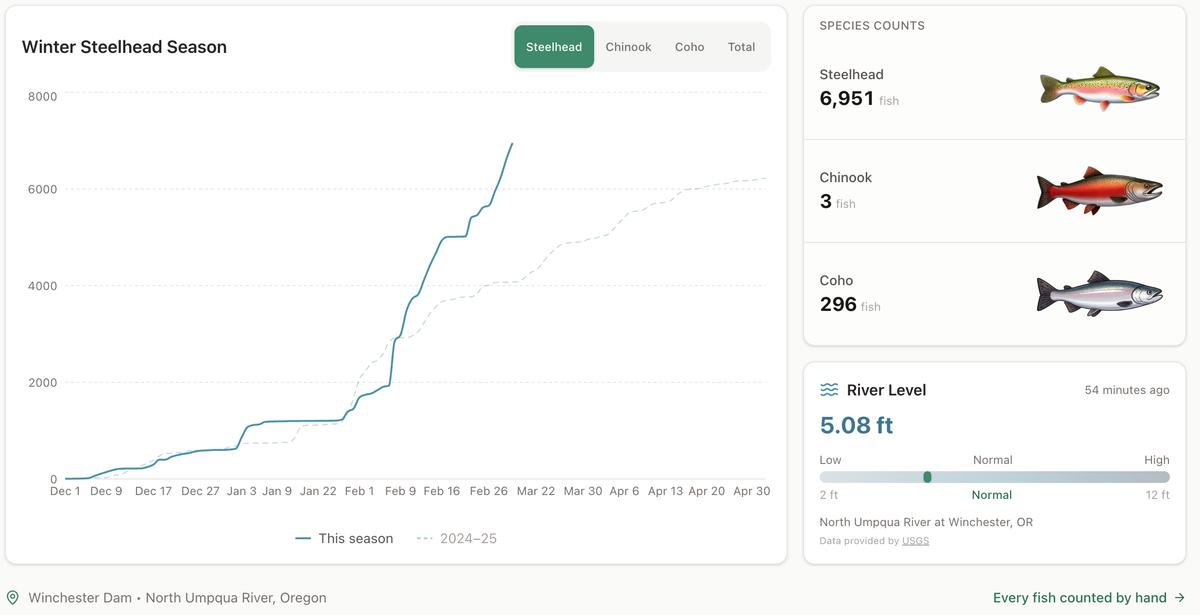
Winter Steelhead Run on the North Umpqua Surpasses Last Year's Total
Nearly 7,000 fish counted at Winchester Dam with two months left in the season
1 min read
Oregon Faces Challenges After Mild Winter
A mild winter has left Oregon with reduced snowpack heading into spring, raising concerns about river levels and insect activity later this year.
1 min read
Stay informed
Get the latest stories from Roseburg Tracker delivered straight to your inbox.